No content results match your keyword.
Content
You have successfully logged out.
Not registered yet?
An exciting technology
Better precision and accuracy, reduced operation time, personal well-being and shorter learning curve.



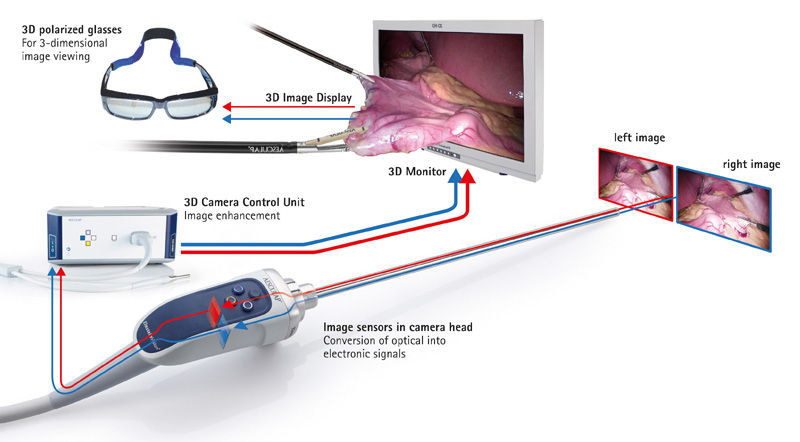




Smaller sensors have a reduced pixel size which usually results in a higher level of disturbing image noise. Therefore it is beneficial to have bigger sensors in the camera.


Laparoscopy has revolutionized surgery compared to open procedures, especially in terms of reducing complications. Laparoscopy can be further improved through innovative technology. One such approach is 3D laparoscopy.
Read moreWhen new medical or technical innovations find their way into general practice, initially there is often not a clear consensus regarding their advantages. The comparison between 3D and 2D laparoscopy, however, has yielded a clear judgment in favor of the 3D technology.
Read moreYour feedback matters! Participate in our customer survey to help us enhance our website, products and services. Thank you for your support!
