No content results match your keyword.
Content
You have successfully logged out.
Not registered yet?
Neurosurgery
The world's leading clips for aneurysm treatment

Based on the development of the aneurysm clip design by the famous Professor Dr. Gazi Yaşargil decades of intensive cooperation with other leading neurosurgeons all over the world formed the foundation for Aesculap’s technical and scientific experience.
With the YASARGIL® Aneurysm Clips, Aesculap is the world market leader. Since their introduction, over 2.0 million clips have been implanted by thousands of neurosurgeons in more than 80 countries. A milestone in the history of neurosurgery and the treatment of cerebral aneurysms. Even though there are alternative treatment options, like coiling, the surgical treatment of unruptered intracranial aneurysms, as well as ruptered aneurysms (subarachnoid hemmorhage / SAH) will represent an important and indispensable therapy option into the future.
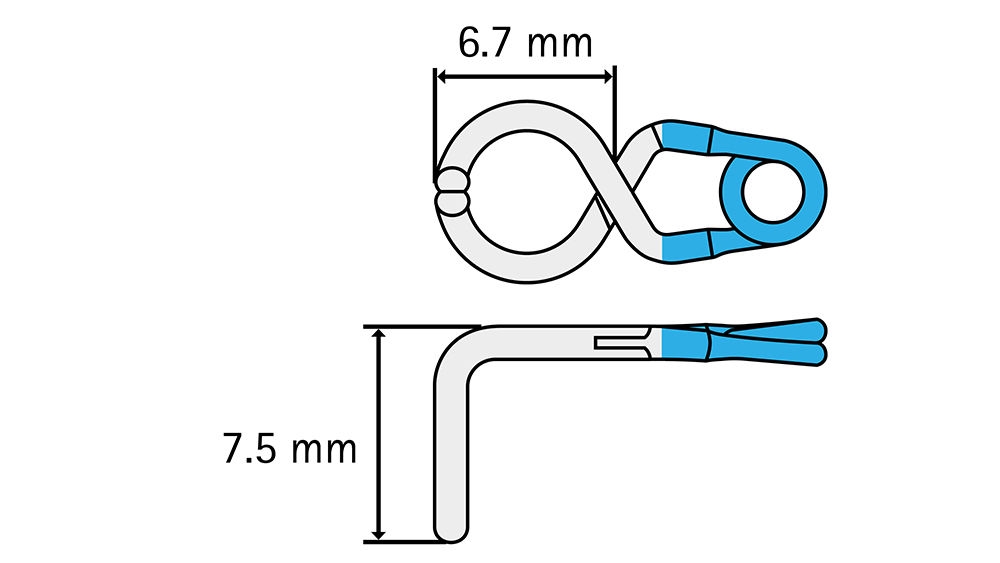
Blade length L1: 7.5 mm
Blade length L2: 6.7 mm
Max. opening: 5.5 mm
Closing force: 1.47 N | 150 g
A 43-year-old woman presented with an unruptured left carotid-ophthalmic aneurysm, unusually arising from the posterior edge of the internal carotid artery. The proximal edge of the neck was very close to the distal dural ring. Adequate surgical exposure required a left anterior clinoidectomy and opening of the left optic canal to access the proximal edge of the neck. The volume of the sack was responsible for a mass effect on the left optical nerve.
The fenestration of the clip was placed around the internal carotid artery, with the blades oriented inferiorly to reach the proximal limit of the neck close to the distal dural ring. The clip provided complete occlusion of the aneurysm and preservation of both internal carotid artery and anterior choroidal artery.
The use of a fenestrated clip allowed the reconstruction of the internal carotid artery without mobilization of the aneurysmal sack which was fragile at some places and adherent to the roof of the cavernous sinus.
There was no other convenient type of clip in our opinion. Neither approaching the clip from the temporal side of the operative field, nor placing a clip between the carotid artery and the optic nerve, which was already severely shifted by the aneurysm, would have been convenient. The only alternative would have been a temporary clipping of the internal carotid artery (at the neck and distal to the aneurysm) to allow the puncture and the deflation of the sack before further dissection of the sack and exclusion with another appropriated clip. The use of a fenestrated clip avoided the temporary occlusion, which otherwise might have been responsible for ischemic complications.






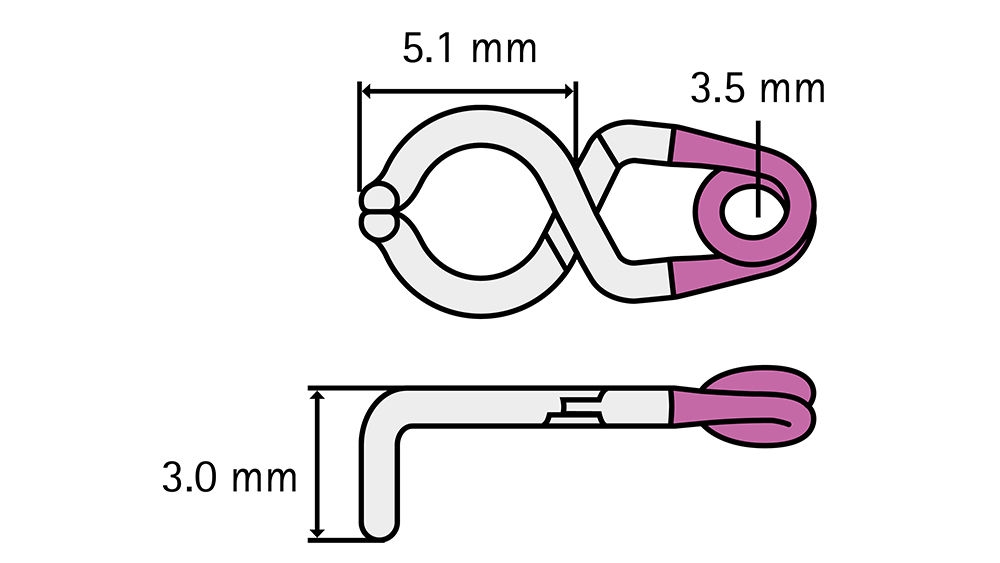
Blade length L1: 3.0 mm
Blade length L2: 5.1 mm
Max. opening: 3.2 mm
Closing force: 1.08 N | 110 g
Diameter of fenestration: 3.5 mm
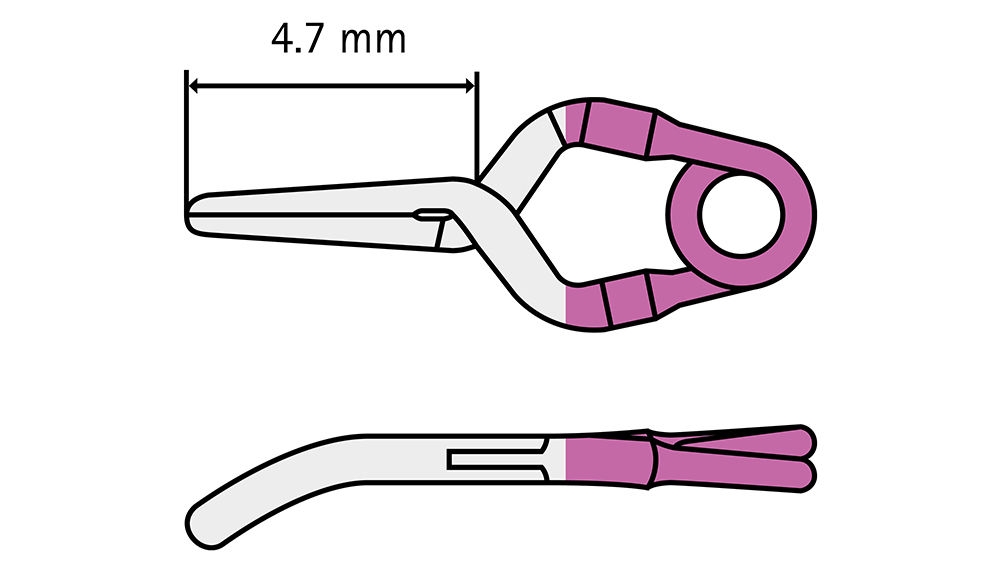
Blade length: 4.7 mm
Max. opening: 3.8 mm
Closing force: 1.08 N | 110 g
Small cerebral aneurysms with narrow neck (3-4 mm in diameter) can be treated by a single clip, leaving no neck remnant. However, for larger cerebral aneurysms (over 5 mm in diameter), such as “dog-ear aneurysms,” a single clip is insufficient to achieve complete occlusion without leaving a neck remnant.
Combined clipping technique: The Yasargil Mini Fenestrated Clip (in this case FT804T) was used to address the issue of neck remnants in larger aneurysms (over 5 mm in diameter) that cannot be completely occluded with a single clip (in this case FT712T).
We used a combined clipping technique with Yasargil fenestrated clips (standard size) to achieve complete neck occlusion in aneurysms with neck remnants. Specifically, dog ear clips FT902T / FT904T are frequently used for neck remnants of 2-3 mm in size and have shown good outcomes. However, these standard size clips need to cross the first clip, and their broad blades create a 0.5 mm triangular gap at the proximal section, which can be problematic if the aneurysm wall is too thin. To address this issue, the Yasargil Mini Fenestrated clips were applied since they have thinner blades and minimize the triangular gap at the proximal section. Additionally, their smaller spring geometry allows their use in locations where larger clips would interfere with surrounding brain tissue and nerves.



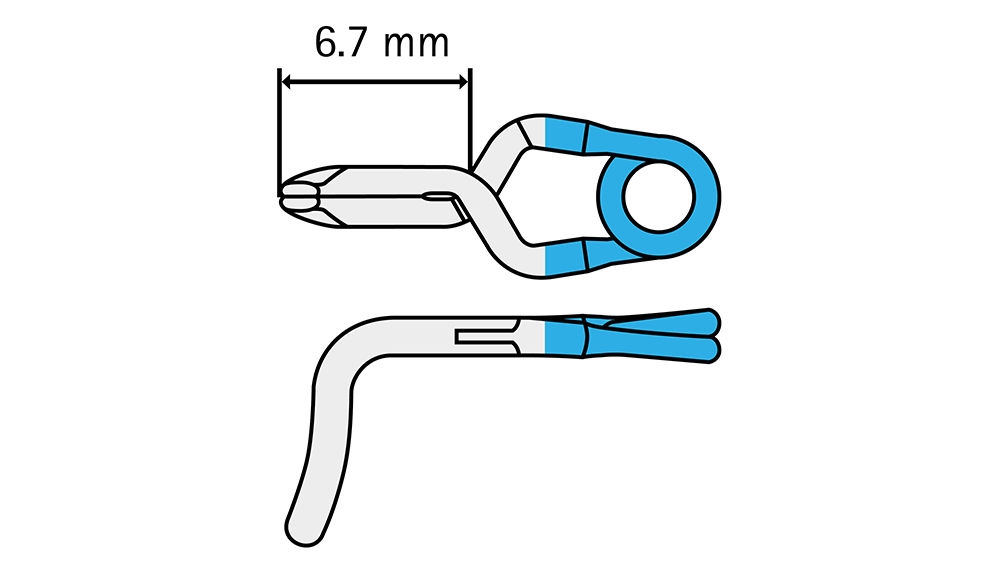
Blade length: 6.7 mm
Max. opening: 5.4 mm
Closing force: 1.96 N | 200 g
53-year-old woman with multiple unruptured intracranial aneurysms diagnosed incidentally. The FT850T clip was used during the surgical clipping of the left middle cerebral artery (MCA), located at the M1-M2 bifurcation. This aneurysm presented itself saccular, slightly irregular, with a diameter of max 5 mm and a neck of 3 mm. The dome was oriented laterally and slightly anteriorly, pointing towards the bottom of the sylvian fissure. The upper part of the dome demonstrated a close relationship with a temporal branch of the dominant inferior division of the M2 segment. The clip was placed right at the neck of the aneurysm, avoiding compression of the M2 divisions.
After careful dissection of the dome of the left MCA-bifurcation aneurysm from the surrounding M2 segments and parenchyma, the arachnoid adhesions were delicately loosened, and the clip was placed in one movement with the blades parallel to the neck of the aneurysm avoiding the two M2 divisions. Before and during the clip placement no temporary clipping was used and after the placement an ICG angiography was performed to check complete closure of the aneurysmal sac and correct filling of the M2 divisions.
In this case the FT850T proved advantageous due to the configuration of the neck of the aneurysm (wide) and its relationship with the minor and major M2 divisions (at the opposite side of the neck). Using the specific curvature of the clip, the primary operator could avoid stenosis of the M2 divisions and also eventual perforators while completely closing the neck of the aneurysm.
This clip proves valuable for aneurysms with a wide neck placed at bifurcations or along a straight parent vessel. It is mostly suited for MCA aneurysms.


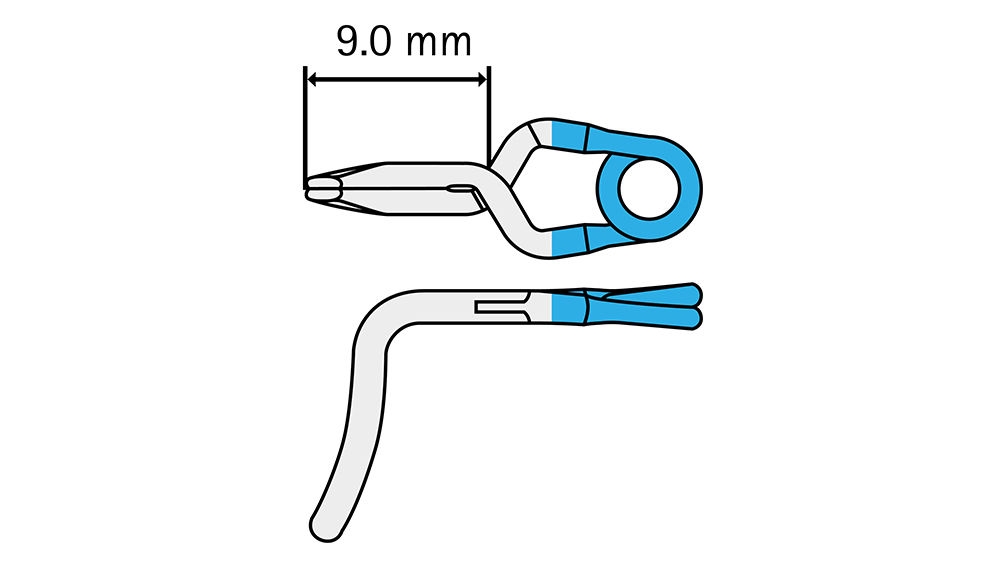
Blade length: 9.0 mm
Max. opening: 5.6 mm
Closing force: 1.96 N | 200 g
A 55-year-old woman was incidentally diagnosed with a 6 mm saccular aneurysm at the left middle cerebral artery (MCA) bifurcation (M1–M2). The aneurysm was slightly irregular, with an estimated neck width of ≈ 5 mm. The dome projected laterally, anteriorly, and slightly superiorly into the Sylvian fissure, and its lateral wall lay close to the inferior M2 division. The clip was placed right at the neck of the aneurysm, avoiding compression of the M2 divisions.
After meticulous dissection of the aneurysm dome from the adjacent M2 branches and surrounding parenchyma, an FT851T clip was applied across the neck. The clip blades were positioned parallel to the neck, carefully avoiding both M2 divisions. Intra-operative flow measurements were taken before clip placement, and temporary proximal clipping was performed with the systolic blood pressure elevated by ≈ 20 % to reduce stroke risk. Indocyanine-green angiography confirmed complete occlusion of the aneurysm sac and unimpaired perfusion of both M2 branches. Post-clipping flow measurements matched pre-clipping values.
The FT851T clip was chosen because its curvature accommodates wide-neck aneurysms situated between the major and minor M2 divisions, allowing secure closure while minimizing the risk of branch stenosis or perforator injury.
Although an FT740T/FT750T (straight) or also an FT42T/FT752T (with the concavity facing below to avoid stenosis of the en passage vessels) could have been considered, the FT851T offered a safer configuration, placed less pressure on the M2 branches and allowed an easier application in this specific case.
Like its shorter counterpart (FT850T), the FT851T is particularly useful for wide-neck aneurysms at arterial bifurcations or along a straight parent vessel, especially within the MCA.


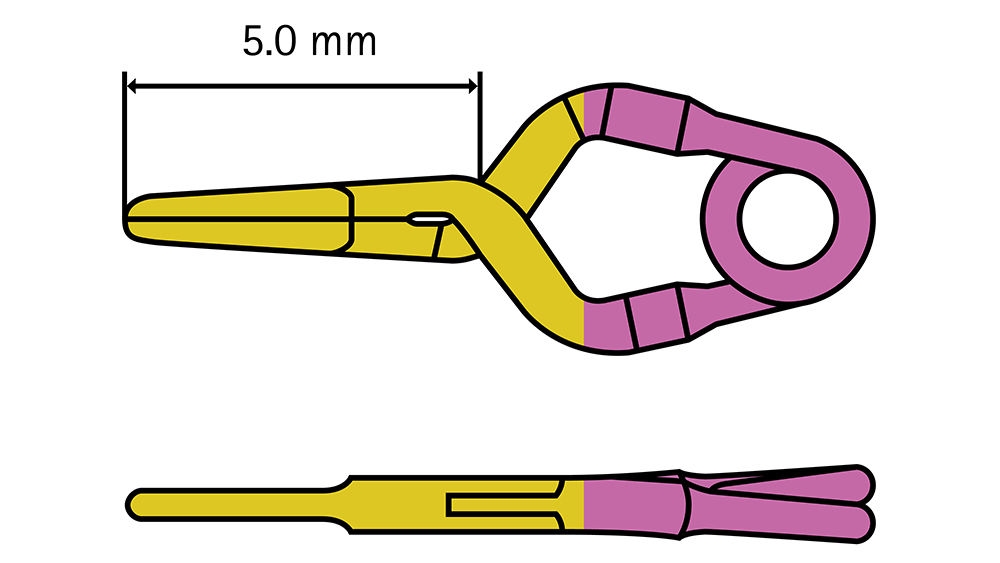
Blade length: 5.0 mm
Max. opening: 4.0 mm
Closing force: 0.69 N | 70 g
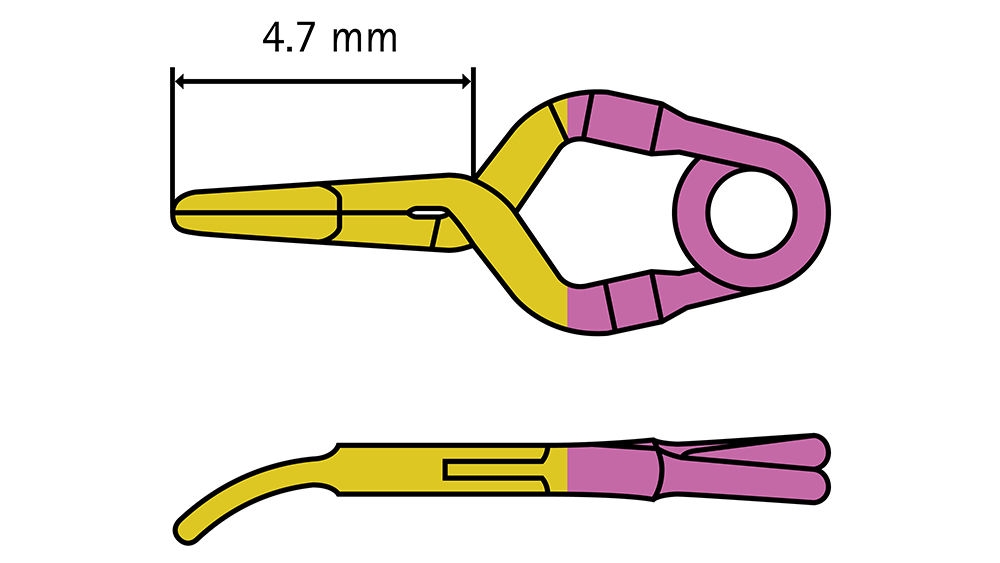
Blade length: 4.7 mm
Max. opening: 3.8 mm
Closing force: 0.69 N | 70 g
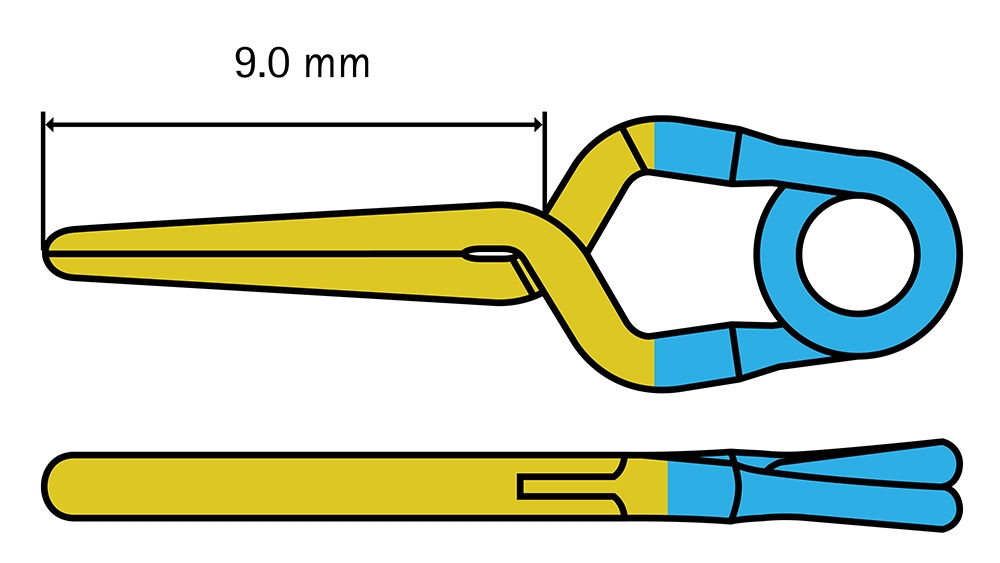
Blade length: 9.0 mm
Max. opening: 7.0 mm
Closing force: 0.88 N | 90 g
This case describes a 36-year-old female diagnosed with Moyamoya disease, characterized by progressive stenosis of the intracranial arteries and recurrent ischemic episodes. The patient underwent a low-flow bypass procedure, connecting the superficial temporal artery (STA) to a cortical branch of the middle cerebral artery (MCA) to restore cerebral perfusion and mitigate ischemic risks.
The STA, a branch of the external carotid artery, was mobilized and prepared for anastomosis with a cortical branch of the MCA, located within the sylvian fissure. Temporary clips were strategically placed to ensure a controlled and bloodless field during the procedure. The FT190T clip was applied to the cortical branch of the MCA to prevent backflow, and the FT250T clip was used on the STA to occlude its flow temporarily during dissection and suturing. Additionally, the FT192T semi-curved clips were employed to achieve temporary occlusion of small perforating branches (medullary arteries) arising from the MCA, minimizing bleeding and ensuring a stable surgical field.
The FT190T clip was chosen for its precision and compatibility with small cortical vessels, ensuring secure occlusion without compromising the integrity of the tissue. The FT250T clip was preferred for its ability to occlude medium-sized vessels like the STA effectively. The FT192T semi-curved clips were essential for managing small perforators, as their curved design facilitated precise positioning, particularly on the inferior surface of the MCA, where perforating branches are commonly situated. This feature minimized the risk of vessel trauma while ensuring effective hemostasis. In this specific case the described clips enhanced surgical precision by maintaining a clear operative field and preventing unnecessary bleeding.
Within the Aesculap catalog, there are several suitable options for temporary vessel occlusion during bypass procedures. For cortical branches of the MCA, other titanium mini clips, such as the FT211T or FT213T, might possibly provide similar performance with slight variations in design for different anatomical requirements. For the STA, straight standard temporary clips, including the FT251T and FT252T, could be considered as conceivable alternatives. When addressing small perforating branches, such as in this specific case, the FT192T semi-curved clip was the optimal choice, although other semi-curved models in the catalog, such as the FT194T, could have been considered. This depends for example on specific vessel positioning and surgical preferences of the respective surgeon.



It will be forwarded to a responsible contact person who will get in touch with you as soon as possible.
Your feedback matters! Participate in our customer survey to help us enhance our website, products and services. Thank you for your support!




