No content results match your keyword.
Content
You have successfully logged out.
Not registered yet?
Solutions beyond fusion
Together with surgeons we worked on the improvement of instruments and surgical techniques: The Ennovate® Cervical system offers surgeons the possibility to achieve optimal surgical outcomes in the occipital, atlantoaxial, subaxial and upper thoracic region.
With our comprehensive spinal system we aim to offer the full range of possibilities – not only with additional navigation, but also for future-oriented technologies like the MIS approach. The system is structured into dedicated instrument modules, so you only open the instrument sets you truly need. Ennovate® Cervical combines next generation implants and instruments with lean process workflows to provide smart solutions for you.
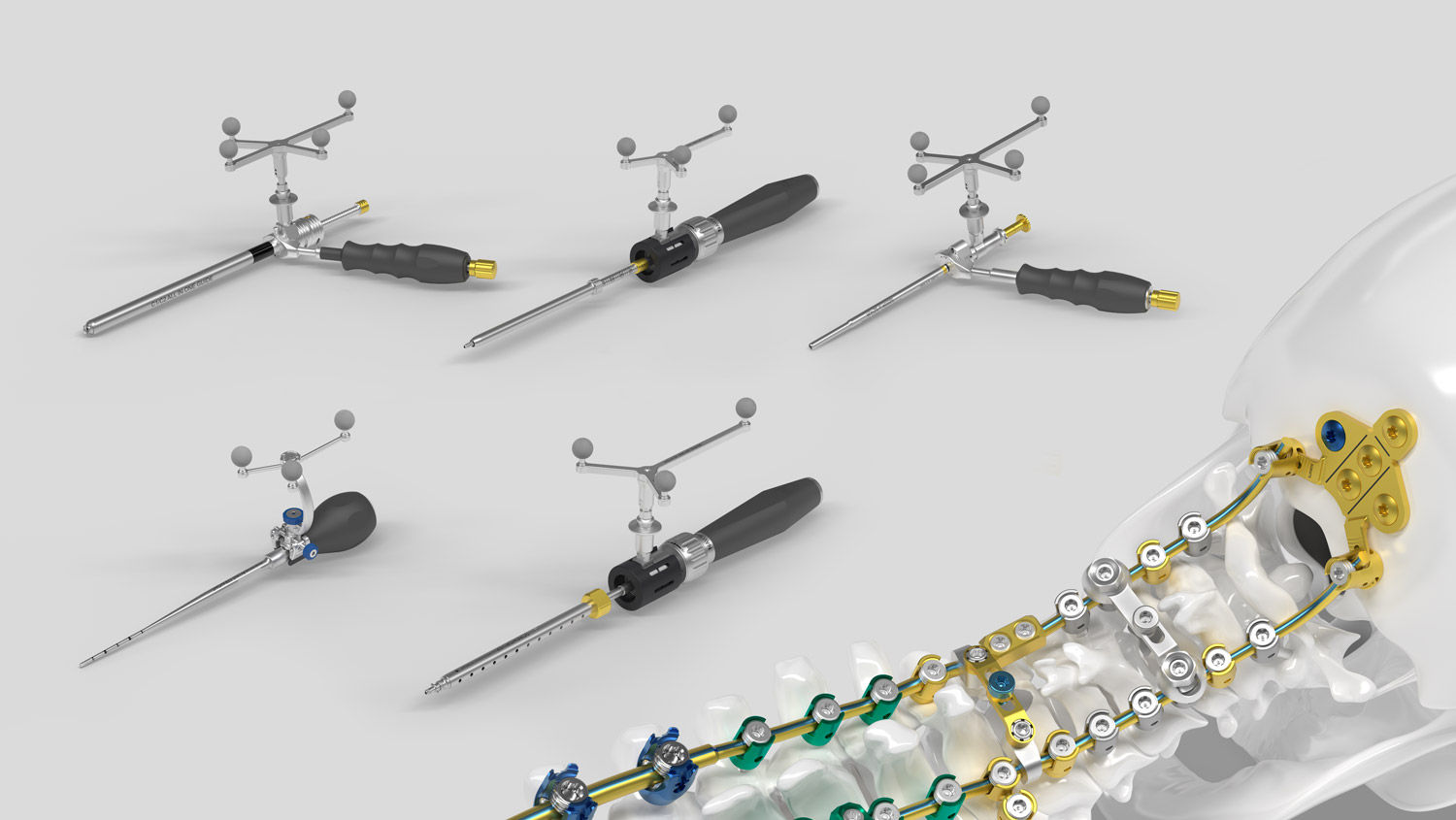
Ennovate® Cervical MIS
Similar to minimally invasive stabilization of the thoracolumbar spine, which have been proposed to reduce access-related morbidity such as muscular denervation, atrophy, length of hospital stay, blood loss and post-operative pain [1-4] procedures for posterior cervical instrumentation represent the next logical step. Several pioneers already reported minimally invasive posterior procedures for stabilization of the cervical spine. [5-9] The MIS module of the Ennovate® Cervical system offers dedicated navigation-ready instruments and implants allowing for a less invasive approach to the cervical spine with the goal to reduce access related morbidity such as post-operative pain.

This first multicenter study demonstrates that fully percutaneous cervical pedicle screw‑rod fixation using 3D navigation is both feasible and safe. Across three centers, 89.7% of screws were placed accurately, with no permanent neurological deficits or wound complications. Accuracy improved over time, indicating a learning curve. Mid‑cervical levels (C3–C6) showed lower accuracy and require particular attention.
Read moreThe study evaluates the feasibility and accuracy of navigated percutaneous cervical pedicle screw instrumentation compared with a matched cohort treated using a conventional open midline approach. The results demonstrate comparable screw placement accuracy between both techniques, while the percutaneous group showed significantly shorter preparation times. Postoperative imaging revealed no relevant differences in paraspinal muscle atrophy between the groups. However, due to the retrospective study design, reliable follow-up imaging was available for only 35–40% of patients, which limits the strength of conclusions regarding muscle preservation. To assess the true benefits of minimally invasive surgery, prospective studies are required. Overall, the findings indicate that the percutaneous approach is a safe and versatile alternative suitable for a broad range of clinical indications.
Read moreThe study compares open versus percutaneous navigated cervical pedicle screw placement for traumatic subaxial cervical spine injuries and shows that both techniques achieve similar accuracy in screw positioning. Percutaneous surgery demonstrated clear advantages, including a significantly shorter operative time (101 min vs. 148 min) and a notably lower intraoperative blood loss (166 mL vs. 342 mL). Further studies are needed to evaluate long-term clinical outcomes.
Read moreThis anatomical feasibility study investigates the accuracy of navigated percutaneous cervical pedicle screw placement in the subaxial cervical spine. In a cadaveric setting, all subaxial cervical pedicles were instrumented using a standardized, navigation‑supported minimally invasive procedure. The results demonstrate that navigated percutaneous cervical pedicle screw placement can be performed with a high level of accuracy under the described conditions, supporting the technical feasibility of this approach.
Read moreA new minimally invasive cervical pedicle screw (CPS) fixation system using intra‑operative computed tomography‑guided navigation This pilot study reports on workflow, feasibility, and accuracy of a minimally invasive surgical (MIS) approach for cervical pedicle screw placement using intra‑operative CT‑guided navigation. A series of ten patients undergoing dorsal MIS cervical instrumentation was retrospectively analysed. Screw placement accuracy and procedure‑related events were assessed using established classification criteria. The results indicate that MIS cervical pedicle screw placement using CT‑based navigation can be performed with acceptable accuracy and appears feasible and safe in selected cases when performed by experienced surgeons.
Read MoreThis retrospective case series included patients with cervical instabilities treated by minimally invasive, percutaneous cervical and upper thoracic spine pedicle screw and rod insertion using Ennovate® Cervical. The results of this study indicate that minimally invasive percutaneous implantation of a pedicle screw-rod system is feasible.
Read MoreSimilar to the thoracic and lumbar spine, minimally invasive surgery (MIS) techniques in the cervical spine aim to achieve outcomes comparable to conventional procedures with regard to target surgery, while at the same time offering the benefits of less traumatic access surgery. In contrast to the thoracic and lumbar regions, however, MIS techniques in the cervical spine are predominantly applied via posterior approaches.
Read More
“With Ennovate® Cervical I have the full range of possibilities for solving complex situations I face in the operating room – It is a truly future-oriented system taking advanced minimally invasive approaches into account.”
Ennovate® performance design
Do you know what happens to the screws post-operatively? Long-term stability is often taken for granted and rarely considered in detail, since it is a primary requirement and assumed that it is technically impossible to get more out of a screw. Because screws are just screws. Well, we do not see it that way! Our German engineers have designed a screw that sets new biomechanical benchmarks.


Ennovate® Cervical EnnoCore
The Ennovate® Cervical implants have a specifically designed screw core and thread shape, all aiming to increase the stability and especially the pull-out strength of the implants. But that´s not all: The drills are harmonized to meet the screw contour and are therefore designed to support better bone compaction and anchorage.
Ennovate® Cervical EnnoTip
The screw tip of the Ennovate® Cervical screw is specially designed to allow for a deeper initial insertion, thereby aiming to reduce the risk of slipping off the prepared bone. Furthermore, the thread starts directly at the screw tip, which is a desing enabling a reduction of the required insertion pressure – critical in the highly mobile cervical spine.

Ennovate® Cervical spinal navigation
The instrumentation is designed to allow for navigation without the need of an additional set of dedicated navigation instruments such as screwdriver or tap. The standard instrumentation may be navigated using the dedicated navigation handles and specifically designed interfaces on the instruments. Reducing the number instruments. Supporting your workflows.
Discover Ennovate®
Your feedback matters! Participate in our customer survey to help us enhance our website, products and services. Thank you for your support!


